 Sanjay Kumar
Sanjay Kumar Alfred Veldhuis
Alfred Veldhuis Tina Malhotra2
Tina Malhotra2- 1Department of Psychology, Oxford Brookes University, Oxford, United Kingdom
- 2Oxford Health Foundation NHS Trust, Oxford, United Kingdom
Coronavirus disease 2019 (COVID-19) is likely to have long-term mental health effects on individuals who have recovered from COVID-19. Rightly, there is a global response for recognition and planning on how to deal with mental health problems for everyone impacted by the global pandemic. This does not just include COVID-19 patients but the general public and health care workers as well. There is also a need to understand the role of the virus itself in the pathophysiology of mental health disorders and longer-term mental health sequelae. Emerging evidence suggests that COVID-19 patients develop neurological symptoms such as headache, altered consciousness, and paraesthesia. Brain tissue oedema and partial neurodegeneration have also been observed in an autopsy. In addition, there are reports that the virus has the potential to cause nervous system damage. Together, these findings point to a possible role of the virus in the development of acute psychiatric symptoms and long-term neuropsychiatric sequelae of COVID-19. The brain pathologies associated with COVID-19 infection is likely to have a long-term impact on cognitive processes. Evidence from other viral respiratory infections, such as severe acute respiratory syndrome (SARS), suggests a potential development of psychiatric disorders, long-term neuropsychiatric disorders, and cognitive problems. In this paper, we will review and evaluate the available evidence of acute and possible long-term neuropsychiatric manifestations of COVID-19. We will discuss possible pathophysiological mechanisms and the implications this will have on preparing a long-term strategy to monitor and manage such patients.
Introduction
Coronaviruses are single-stranded RNA viruses, which caused two well-known outbreaks: (1) severe acute respiratory syndrome (SARS) in 2002 and (2) Middle East respiratory syndromes (MERS) in 2012. Since December 2019, several cases of atypical pneumonia have been reported from Wuhan, China. A novel coronavirus was identified to be the cause and was subsequently named by the WHO as: “severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).” It is well known that coronaviruses affect the respiratory tract, with most patients experiencing only mild symptoms akin to the common cold (e.g., blocked/runny nose, headaches, sneezing, a raised temperature, loss of taste and smell, etc.) and the illness is self-limiting. However, if the virus reaches lower respiratory tract, in vulnerable individuals such as new-born, elderly, and immunocompromised, it can cause severe illness such as pneumonia, bronchitis, exacerbation of asthma, chronic obstructive pulmonary disease (COPD), and acute respiratory syndrome (ARS), as seen in SARS, MERS, and now COVID-19 (Desforges et al., 2014; Raj et al., 2014). Unfortunately, coronavirus is an opportunistic virus and can allude immune response, potentially spreading to cells other than the respiratory tract’s epithelial cells. Several coronaviruses have shown to be neuro-invasive, including SARS and MERS (Gu et al., 2005; Xu et al., 2005; Arabi et al., 2015).
As of the 28th of June 2020, SARS-CoV-2 has now infected over 10 million people worldwide (Dong et al., 2020) and the pandemic continues to grow. The disease caused by SARS-CoV-2 is known as corona virus disease 2019 (COVID-19), which manifests not just as a respiratory illness but also impacts the cardiovascular, renal, and the nervous system functions (Yuki et al., 2020). It is known from previous pandemics, such as Spanish influenza and SARS, that there are not just acute effects of the viral infection but also long-term sequelae due to disease itself as well as social effects due to governmental measures of containment such as quarantine, social distancing, and lockdown.
In this paper, we aim to present an understanding of pathophysiology, possible effects of SARS-CoV-2 infection to the brain and its long-term neuropsychiatric and cognitive consequences. Understanding neuropsychiatric and cognitive consequences are important, as millions of individuals have been affected; many more are undetected, and the number of infections is still rising. If even a fraction of such individuals experience neuropsychiatric complications, the public health implications could be considerable. Therefore, it is important to understand the neuropsychiatric and cognitive consequences of COVID-19. In this paper, we will briefly outline how COVID-19 can affect the central nervous system (CNS), review emerging evidence of effects on CNS and explore the possible neuropsychiatric sequelae of the COVID-19 infection. We will discuss diverse neuropsychiatric and cognitive complications following COVID-19 infection, possibly affecting a large proportion of individuals previously suffering from COVID-19. This, in turn, could lead to a potential increase in patients with psychiatric and cognitive problems. Understanding and assessing cognitive consequences following COVID-19 is important as it could be used to estimate an individual’s capacity to work effectively, drive, manage finances, participate in daily family activities, or make informed decisions. Appropriate neuropsychological rehabilitation could beplanned to remediate or compensate for cognitive deficits in COVID-19 survivors.
Neuropsychiatric consequences are neurological, psychiatric, and cognitive problems due to direct brain damage, disease, or indirect effects on the CNS via an immune response or medical therapy (Rogers et al., 2020). The acute psychiatric manifestations of COVID-19 reported in surveys are increased stress, anxiety, and depression (Asmundson and Taylor, 2020). In the long-term, psychiatric presentations could also be affected by the outcome of their illness, stigma or memories, and amnesia associated with the critical care they receive (Jones et al., 1998). Acute neurological symptoms such as headache, altered sensorium, acute cerebrovascular incidents, convulsions, and ataxia have been reported in more than a third of hospitalized patients (Mao et al., 2020). Reports of acute cognitive complications such as attention and dysexecutive symptoms are also emerging (Rogers et al., 2020; Varatharaj et al., 2020). However, we can just speculate about the long-term neuropsychiatric and cognitive consequences of COVID-19.
Pathophysiology of Neuropsychiatric and Cognitive Consequences of Covid-19
SARS-CoV-2 is a novel virus and its pathophysiological mechanism on various physiological systems is yet to be fully understood. However, a lot can be learnt from other subtypes of coronaviruses. Coronaviruses primarily affect upper respiratory tracts, but they have been detected both in the brain and cerebrospinal fluids of the infected individuals (Bohmwald et al., 2018). There are several mechanisms through which coronaviruses can damage the nervous system. These may include direct infection injury, virus entering through blood circulation pathway, neuronal pathway, hypoxic injury, immune injury, and via binding to the angiotensin-converting enzyme 2 (ACE2). The neurotropic capacities of coronaviruses allow them to evade the immune response of the host and achieve latency. This makes them a potent factor to cause acute and late neurological effects. Although early indication shows that the expression of SARS-CoV-2 in the brain deviates slightly compared to SARS-CoV-1 and MERS expression, it is still a potential source for causing short and long-term neuropsychiatric and cognitive complications. For a detailed discussion of these mechanisms, please see Wu et al. (2020). The neuronal pathway via the olfactory nerve and role of ACE2 has been observed to be the primary pathophysiological mechanisms contributing to neuropsychiatric and cognitive complications in COVID-19 (Mirfazeli et al., 2020; Pantelis et al., 2020). This is mainly because coronaviruses affect the respiratory tract and can reach the ACE2-enzymes in the respiratory epithelial cells, and the olfactory nerve, providing a pathway for the coronavirus to enter the CNS.
Neuronal Pathway
Neurotropic viruses, such as coronaviruses, use sensory and motor neuronal pathways to enter the CNS. One example of a neuronal pathway is the olfactory nerve (Desforges et al. 2019). This is mediated by the unique organization of olfactory nerves and the olfactory bulb in the nasal cavity and forebrain. The virus thus can reach the brain and CSF, which can cause inflammation and a demyelinating reaction. If the infection is set, then the viruses can reach the whole brain and CSF in less than 7 days (Bohmwald et al., 2018). Altered olfaction and gustatory problems (anosmia, hyposmia, and ageusia) have been reported in 49% of COVID-19 patients (Hornuss et al., 2020; Vaira et al., 2020) implicating the possibility of CNS infection through the olfactory neuronal pathway.
ACE2 and Its Role in Neuropsychiatric Complications
ACE2 enzyme is widely present in various organs including oro-nasal, respiratory, cardiovascular, cerebrovascular, and immune systems. The high density of ACE2 in oro-nasal mucosa and their binding with SARS-CoV-2 may account for olfactory symptoms of anosmia in COVOD-19 (Lechien et al., 2020). Coronaviruses directly bind to ACE-2 receptors in respiratory epithelial cells cause cytokine storm, which causes widespread inflammation in patients with COVID-19, leading to multiple organ damage and immune-mediated encephalopathy manifesting as delirium and convulsions. Neuroinflammation is a well-recognized mechanism for the development of psychiatric disorders (Yuan et al., 2019). It can also cause hypercoagulable states causing ischaemic stroke besides other vascular events (Fotuhi et al., 2020). ACE2 plays an important role in controlling blood pressure but binding to SARS-CoV-2 can cause an increase in blood pressure, which can increase the propensity to cerebral hemorrhage. This may also explain the increase in mortality in patients with COVID-19 with comorbid metabolic conditions such as hypertension, high body mass index and diabetes (Fang et al., 2020). It has also been proposed that the spike protein of SARS-CoV-2 can bind to ACE2 receptors in capillaries, breaking the blood-brain barrier and allowing the virus to enter the brain directly (Wu et al., 2020). Neurons have a high density of ACE-2 and high binding to coronaviruses if they cross the blood-brain barrier. SARS-CoV-2 can lie latent in the neurons of patients who recover from acute effects of COVID-19, increasing the risk of long-term consequences by causing demyelination and neurodegeneration (Lippi et al., 2020).
Neuropsychiatric and Cognitive Effects of Coronavirus Infection
Acute Effects
In the short-term, 20–40% of COVID-19 cases may present with neuropsychiatric complications, such as cerebrovascular events, headache, dizziness, encephalopathies, anosmia, ageusia, and mood problems (Bo et al., 2020; Crunfli et al., 2020; Lu et al., 2020; Mao et al., 2020; Mirfazeli et al., 2020; Troyer et al., 2020; Varatharaj et al., 2020; Wu et al., 2020; Zhang et al., 2020), see Table 1. The acute effect of CoV infections on the CNS is manifested in viral encephalitis, infectious toxic encephalopathy, and acute cerebrovascular disease. In a recent meta-analytic review, Rogers et al. (2020) reported the neuropsychiatric short- and long-term consequences of SARS and MERS infection. They reported that during the acute illness, 27–41% of cases had neuropsychiatric symptoms such as confusion, depressed mood, anxiety, impaired memory, and insomnia. Steroid-induced mania and psychoses were also reported. The meta-analysis also looked at the available data related to COVID-19 infection and neuropsychiatric consequences and found that confusion and agitation were present in 65–69% of the intensive care unit patients. Importantly, at discharge, 33% of the patients with COVID-19 had dysexecutive syndromes. Similarly, in a United Kingdom wide surveillance study, 153 patients were reported to have neurological and neuropsychiatric complications following COVID-19 infection (Varatharaj et al., 2020). Twenty-one of these cases developed a new diagnosable psychiatric disorder. The other noteworthy observation was the effect of age on altered mental status and cerebrovascular incident. Thirty-seven patients had altered mental status and 49% of these patients were younger than 60 years. However, of 74 patients who presented with cerebrovascular incidents, 81% of the patients were aged over 60. In another report, Mao et al. (2020) reported neurologic manifestations of COVID-19. The study had 214 patients with mild to severe COVID-19 infection. Around 36.4% of the patients showed neurologic manifestations involving the CNS, peripheral nervous system (PNS) and skeletal muscles. These neurologic manifestations were more prevalent in patients with a severe infection and included signs of impaired consciousness and acute cerebrovascular diseases. Autopsy results have indicated degenerated neurons and an increased blood flow to some regions together with edematous brain tissue (Mao et al., 2020).
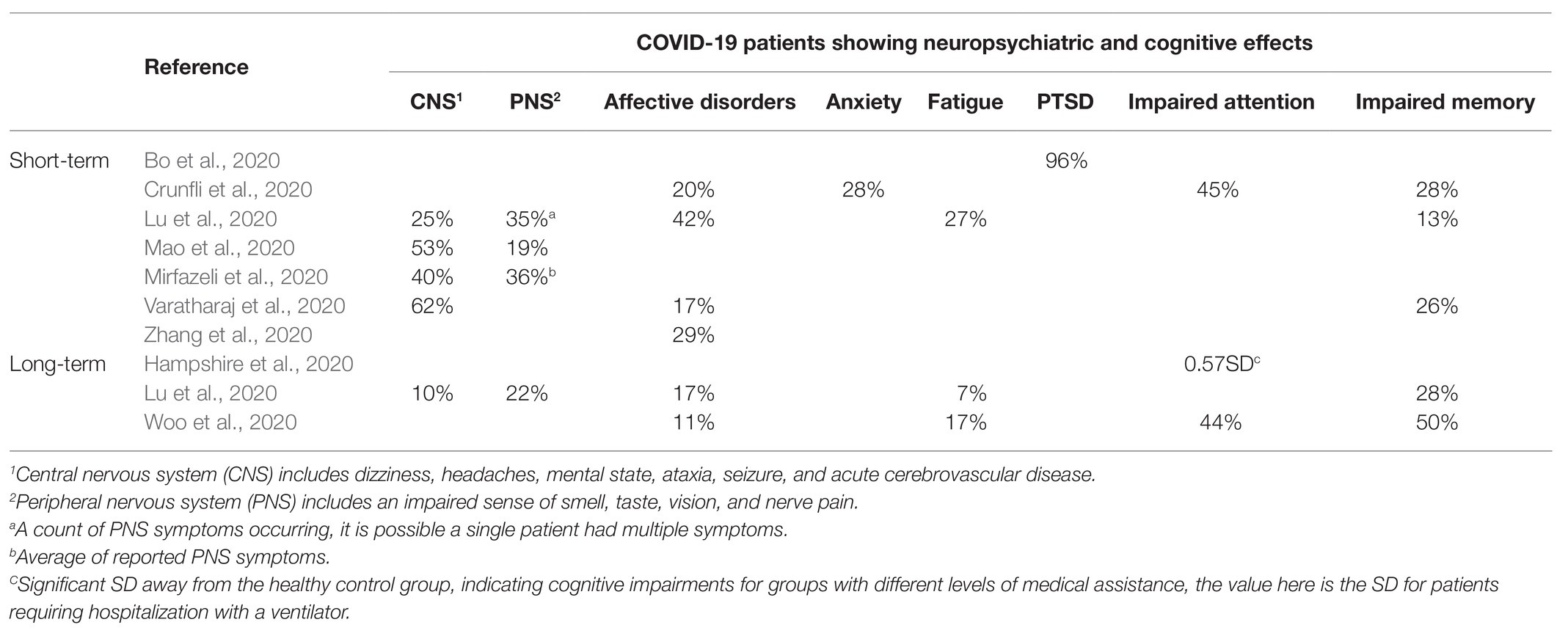
Table 1. Percentage of COVID-19 patients showing neuropsychiatric and cognitive effects.
Structural brain abnormalities have also been reported with SARS-CoV-1 and MERS infections. In an MRI study looking into the post-infectious neurological consequences of MERS in three patients with severe neurologic syndrome found hyperintensities in the white matter of the parietal lobes, temporal lobes, frontal lobes, basal ganglia, and corpus callosum (Arabi et al., 2015). The neurological manifestations shown by these patients included: altered mental status (ranging from confusion to coma) ataxia, and focal motor deficits. Similarly, a study investigating autopsies of six SARS patients found evidence of edema and scattered red degeneration of the neurons (likely the result of neuronal hypoxia or ischemia), after finding evidence of SARS genome sequences in the hypothalamus and cortex (Gu et al., 2005). Structural brain abnormalities have been reported in COVID-19 patients too. Montalvan et al. (2020) have reported cases with brain abnormalities present in the bilateral thalamic, medial temporal lobes, hippocampus, and insular regions.
As reported by Helms et al. (2020), there are some findings of encephalopathy and reduced blood flow in the frontotemporal brain region following a COVID-19 infection. The extent to which COVID-19 infection leads to neurological damages and neuronal symptoms is currently still unknown. However, several studies have found patients with neurological diseases ranging from encephalitis to strokes (Mao et al., 2020; Moriguchi et al., 2020). Encephalitis alone is linked to an increased risk of a range of long-term sequelae such as epilepsy, bipolar disorders, psychotic disorders, anxiety disorders, cognitive problems, and dementia (Granerod et al., 2017).
Long-Term and Chronic Neuropsychiatric Sequelae
It is known that the neural and immune cells can host latent CoV which could contribute to delayed neurologic and neuropsychiatric complications (Desforges et al., 2019). However, long-term neuropsychiatric sequelae of COVID-19 are currently unknown. We can speculate long-term effects from our understanding of the mechanisms of the COVID-19 on the CNS and evidence from long-term neuropsychiatric effects of SARS-CoV-1 and MERS. Lam et al. (2009) reported that 55% of survivors of SARS-CoV-1 had post-traumatic stress disorder (PTSD). Furthermore, depression was in 39%, pain disorder in 36.4%, panic disorder in 32.5%, and obsessive-compulsive disorder in 15.6% of SARS-CoV-1 survivors. In their meta-analytic review, Rogers et al. (2020) also reported long-term neuropsychiatric consequences of SARS and MERS infections in 10–20% of the cases, such as depressed mood, insomnia, anxiety, irritability, memory impairment, and fatigue. However, it is important to understand that the neuropsychiatric manifestations, such as PTSD, depression, or anxiety, following COVID-19 infection could also be a psychological reaction to being infected, being in intensive care unit or experiencing stigma of contracting the infection.
If similar proportions of long-term neuropsychiatric complications emerge following COVID-19, then we can expect a crashing wave of neuropsychiatric sequelae (Troyer et al., 2020), which will have huge implication for management of the stretched healthcare resources in every country. Besides the neuropsychiatric sequelae, long-term implications will be observed with many neurological problems. For example, loss of smell is considered one of the hallmark symptoms of COVID-19 infection implying CNS involvement. This might have long-term implications for neuro infections and neurodegenerative diseases. Indeed, loss of olfaction is considered an early manifestation in Parkinson’s disease (Doty, 2012; Chase and Markopoulou, 2020). Therefore, the emergence of cognitive symptoms following COVID-19 may indicate an underlying neurodegenerative process. Furthermore, individuals with certain immunocompromised neurological conditions such as multiple sclerosis (MS) may show alterations in their non-motor symptoms following COVID-19, which may indicate an underlying neurodegenerative process. Higher risk of developing Parkinson’s disease and MS has been previously linked to SARS-CoV-1 infection (Fazzini et al., 1992; Murray et al., 1994). Indeed, long-term assessment of cognition will become a critical part of the care pathway for such individuals.
Long-Term Cognitive Sequelae
From the emerging evidence and our understanding of the mechanism of CoV in the CNS, one can expect to have a range of cognitive consequences of COVID-19 infection. Attention and dysexecutive symptoms have commonly been reported with COVID-19 (Rogers et al., 2020; Varatharaj et al., 2020). Hypoperfusion in the frontotemporal region of the brain has also been reported (Helms et al., 2020) as well as structural brain abnormalities thalamic and temporal regions (Montalvan et al., 2020). Considering the demyelinating nature of the viral infection in the CNS, we can expect common cognitive problems that characterize demyelinating illnesses (such as MS). The Symbol Digit Modalities Test (SDMT), a test to assess the speed of information processing, is an exceptionally reliable and sensitive cognitive test for MS patients (Benedict et al., 2017). Similarly, a link between loss of smell in COVID-19 patients and the prodromal phase of Parkinson’s disease should be kept in mind while examining long-term cognitive consequences. A large amount of research has shown that executive functions are primarily affected in the prodromal phase of Parkinson’s disease along with prominent memory problems (Fengler et al., 2017). Taken together, the long-term cognitive examination of COVID-19 survivors should at least include tests assessing attention, executive functions, learning, and memory as well as the speed of information processing.
Implications for Monitoring Long-Term Neuropsychiatric and Cognitive Sequelae
It is clear from the past outbreaks of SARS-CoV-1 and MERS and current reports of neurological and neuropsychiatric complications following COVID-19 that a large number of survivors will experience a range of neuropsychiatric and cognitive sequelae. These are likely to affect their mental, physical, and cognitive well-being. Which, in turn, will affect their emotional, occupational, and financial situations. Some of these patients may develop a full-blown neurological or psychiatric illness, or some might experience mild cognitive problems and that will increase their risk of developing dementia. Early indications show that the cognitive domains of executive functions, attention, and memory appear to be affected by COVID-19. Furthermore, there are potential increases in affective disorders, anxiety, fatigue, and PTSD (Hampshire et al., 2020; Lu et al., 2020; Woo et al., 2020), see Table 1. These symptoms can be due to pathoplastic change in brain physiology where the COVID-19 infection may modify brain functions after infection, which can lead to the development of brain vulnerabilities that may increase the probability to develop psychological distress. It is also possible that these neuropsychiatric symptoms and disorders are the psychological reactions of having contracted COVID-19 and undergoing associated medical interventions. This complex nature of neuropsychiatric presentations can be understood through a careful study of case history, accompanied by standardized neuropsychological assessments. This will help clarify if the neuropsychiatric and cognitive problems are a direct consequence of structural brain abnormalities or are a psychological reaction of the potential physical and the mental stress associated with recovering from COVID-19. Therefore, early detection and prevention of neuropsychiatric and cognitive problems should be the long-term aim of health services and governments across the world as this could present as a “third wave” of the pandemic.
Conclusion
The short-term neuropsychiatric and cognitive complications following COVID-19 are varied and affect a large proportion of COVID-19 survivors. In the medium- and long-term period, there is going to be an influx of patients with psychiatric and cognitive problems who were otherwise healthy prior to COVID-19 infection. Increased neuropsychiatric manifestations could be observed in the form of an increase in cases of depression, anxiety, PTSD, and in certain cases severe mental illnesses. Cognitive sequelae are also likely to be varied and a detailed cognitive evaluation should be considered for such individuals to monitor the emergence of new neurological cases. Robust neuropsychiatric and cognitive monitoring will enable health care providers to plan adequate health care delivery and allocate resources adequately. Early intervention for emerging cognitive problems will be critical for independent functioning and improved quality of life for many COVID-19 survivors.
Author Contributions
All authors participated in the literature search, manuscript preparation, and feedback on final manuscript. SK led the process and conceptualized the topic. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Arabi, Y. M., Harthi, A., Hussein, J., Bouchama, A., Johani, S., Hajeer, A. H., et al. (2015). Severe neurologic syndrome associated with Middle East respiratory syndrome corona virus (MERS-CoV). Infection 43, 495–501. doi: 10.1007/s15010-015-0720-y
Asmundson, G. J. G., and Taylor, S. (2020). Coronaphobia: fear and the 2019-nCoV outbreak. J. Anxiety Disord. 70:102196. doi: 10.1016/j.janxdis.2020.102196
Benedict, R. H. B., DeLuca, J., Enzinger, C., Geurts, J. J. G., Krupp, L. B., and Rao, S. M. (2017). Neuropsychology of multiple sclerosis: looking back and moving forward. J. Int. Neuropsychol. Soc. 23, 832–842. doi: 10.1017/S1355617717000959
Bo, H. -X., Li, W., Yang, Y., Wang, Y., Zhang, Q., Cheung, T., et al. (2020). Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol. Med. 1–2. doi: 10.1017/S0033291720000999 [Epub ahead of print]
Bohmwald, K., Gálvez, N. M. S., Ríos, M., and Kalergis, A. M. (2018). Neurologic alterations due to respiratory virus infections. Front. Cell. Neurosci. 12:386. doi: 10.3389/fncel.2018.00386
Chase, B. A., and Markopoulou, K. (2020). Olfactory dysfunction in familial and sporadic Parkinson’s disease. Front. Neurol. 11:447. doi: 10.3389/fneur.2020.00447
Crunfli, F., Carregari, V. C., Veras, F. P., Vendramini, P. H., Fragnani Valença, A. G., Leão Marcelo Antunes, A. S., et al. (2020). SARS-CoV-2 infects brain astrocytes of COVID-19 patients and impairs neuronal viability. medRxiv [Preprint]. doi: 10.1101/2020.10.09.20207464
Desforges, M., Le Coupanec, A., Dubeau, P., Bourgouin, A., Lajoie, L., Dubé, M., et al. (2019). Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses 12:14. doi: 10.3390/v12010014
Desforges, M., Le Coupanec, A., Stodola, J. K., Meessen-Pinard, M., and Talbot, P. J. (2014). Human coronaviruses: viral and cellular factors involved in neuroinvasiveness and neuropathogenesis. Virus Res. 194, 145–158. doi: 10.1016/j.virusres.2014.09.011
Dong, E., Du, H., and Gardner, L. (2020). An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 20, 533–534. doi: 10.1016/S1473-3099(20)30120-1
Doty, R. L. (2012). Olfaction in Parkinson’s disease and related disorders. Neurobiol. Dis. 46, 527–552. doi: 10.1016/j.nbd.2011.10.026
Fang, L., Karakiulakis, G., and Roth, M. (2020). Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 8:e21. doi: 10.1016/S2213-2600(20)30116-8
Fazzini, E., Fleming, J., and Fahn, S. (1992). Cerebrospinal fluid antibodies to coronavirus in patients with Parkinson’s disease. Mov. Disord. 7, 153–158. doi: 10.1002/mds.870070210
Fengler, S., Liepelt-Scarfone, I., Brockmann, K., Schäffer, E., Berg, D., and Kalbe, E. (2017). Cognitive changes in prodromal Parkinson’s disease: a review. Mov. Disord. 32, 1655–1666. doi: 10.1002/mds.27135
Fotuhi, M., Mian, A., Meysami, S., and Raji, C. A. (2020). Neurobiology of COVID-19. J. Alzheimers Dis. 76, 3–19. doi: 10.3233/JAD-200581
Granerod, J., Davies, N. W. S., Ramanuj, P. P., Easton, A., Brown, D. W. G., and Thomas, S. L. (2017). Increased rates of sequelae post-encephalitis in individuals attending primary care practices in the United Kingdom: a population-based retrospective cohort study. J. Neurol. 264, 407–415. doi: 10.1007/s00415-016-8316-8
Gu, J., Gong, E., Zhang, B., Zheng, J., Gao, Z., Zhong, Y., et al. (2005). Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 202, 415–424. doi: 10.1084/jem.20050828
Hampshire, A., Trender, W., Chamberlain, S., Jolly, A., Grant, J. E., Patrick, F., et al. (2020). Cognitive deficits in people who have recovered from COVID-19 relative to controls: an N=84,285 online study. medRxiv [Preprint]. doi: 10.1101/2020.10.20.20215863
Helms, J., Kremer, S., Merdji, H., Clere-Jehl, R., Schenck, M., Kummerlen, C., et al. (2020). Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 382, 2268–2270. doi: 10.1056/NEJMc2008597
Hornuss, D., Lange, B., Schröter, N., Rieg, S., Kern, W. V., and Wagner, D. (2020). Anosmia in COVID-19 patients. Clin. Microbiol. Infect. 26, 1426–1427. doi: 10.1016/j.cmi.2020.05.017
Jones, C., Humphris, G. M., and Griffiths, R. D. (1998). Psychological morbidity following critical illness - the rationale for care after intensive care. Clin. Intensive Care 9, 199–205. doi: 10.3109/tcic.9.5.199.205
Lam, M. H. B., Wing, Y. K., Yu, M. W. M., Leung, C. M., Ma, R. C. W., Kong, A. P. S., et al. (2009). Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors long-term follow-up. Arch. Intern. Med. 169, 2142–2147. doi: 10.1001/archinternmed.2009.384
Lechien, J. R., Chiesa-Estomba, C. M., De Siati, D. R., Horoi, M., Le Bon, S. D., Rodriguez, A., et al. (2020). Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur. Arch. Otorhinolaryngol. 277, 2251–2261. doi: 10.1007/s00405-020-05965-1
Lippi, A., Domingues, R., Setz, C., Outeiro, T. F., and Krisko, A. (2020). SARS-CoV-2: at the crossroad between aging and Neurodegeneration. Mov. Disord. 35, 716–720. doi: 10.1002/mds.28084
Lu, Y., Li, X., Geng, D., Mei, N., Wu, P. -Y., Huang, C. -C., et al. (2020). Cerebral micro-structural changes in COVID-19 patients – an MRI-based 3-month follow-up study. EClinicalMedicine 25:100484. doi: 10.1016/j.eclinm.2020.100484
Mao, L., Jin, H., Wang, M., Hu, Y., Chen, S., He, Q., et al. (2020). Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 77, 683–690. doi: 10.1001/jamaneurol.2020.1127
Mirfazeli, F. S., Sarabi-Jamab, A., Jahanbakhshi, A., Kordi, A., Javadnia, P., Shariat, S. V., et al. (2020). Neuropsychiatric manifestations of COVID-19 can be clustered in three distinct symptom categories. Sci. Rep. 10:20957. doi: 10.1038/s41598-020-78050-6
Montalvan, V., Lee, J., Bueso, T., De Toledo, J., and Rivas, K. (2020). Neurological manifestations of COVID-19 and other coronavirus infections: a systematic review. Clin. Neurol. Neurosurg. 194:105921. doi: 10.1016/j.clineuro.2020.105921
Moriguchi, T., Harii, N., Goto, J., Harada, D., Sugawara, H., Takamino, J., et al. (2020). A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 94, 55–58. doi: 10.1016/j.ijid.2020.03.062
Murray, R. S., Cai, G. Y., Hoel, K., Johnson, S., and Cabirac, G. F. (1994). Coronaviruses and multiple sclerosis. Adv. Exp. Med. Biol. 342, 353–357. doi: 10.1007/978-1-4615-2996-5_54
Pantelis, C., Jayaram, M., Hannan, A. J., Wesselingh, R., Nithianantharajah, J., Wannan, C. M., et al. (2020). Neurological, neuropsychiatric and neurodevelopmental complications of COVID-19. Aust. N. Z. J. Psychiatry 0004867420961472. doi: 10.1177/0004867420961472 [Epub ahead of print]
Raj, V. S., Osterhaus, A. D. M. E., Fouchier, R. A. M., and Haagmans, B. L. (2014). MERS: emergence of a novel human coronavirus. Curr. Opin. Virol. 5, 58–62. doi: 10.1016/j.coviro.2014.01.010
Rogers, J. P., Chesney, E., Oliver, D., Pollak, T. A., McGuire, P., Fusar-Poli, P., et al. (2020). Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 7, 611–627. doi: 10.1016/S2215-0366(20)30203-0
Troyer, E. A., Kohn, J. N., and Hong, S. (2020). Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav. Immun. 87, 34–39. doi: 10.1016/j.bbi.2020.04.027
Vaira, L. A., Salzano, G., and Deiana, G., and De Riu, G. (2020). Anosmia and Ageusia: common findings in COVID-19 patients. Laryngoscope 130:1787. doi: 10.1002/lary.28692
Varatharaj, A., Thomas, N., Ellul, M., Davies, N. W. S., Pollak, T., Tenorio, E. L., et al. (2020). UK-wide surveillance of neurological and neuropsychiatric complications of COVID-19: The first 153 patients. SSRN [Preprint]. doi: 10.2139/ssrn.3601761
Woo, M. S., Malsy, J., Pöttgen, J., Seddiq Zai, S., Ufer, F., Hadjilaou, A., et al. (2020). Frequent neurocognitive deficits after recovery from mild COVID-19. Brain Commun. 2:fcaa205. doi: 10.1093/braincomms/fcaa205
Wu, Y., Xu, X., Chen, Z., Duan, J., Hashimoto, K., Yang, L., et al. (2020). Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 87, 18–22. doi: 10.1016/j.bbi.2020.03.031
Xu, J., Zhong, S., Liu, J., Li, L., Li, Y., Wu, X., et al. (2005). Detection of severe acute respiratory syndrome coronavirus in the brain: potential role of the chemokine mig in pathogenesis. Clin. Infect. Dis. 41, 1089–1096. doi: 10.1086/444461
Yuan, N., Chen, Y., Xia, Y., Dai, J., and Liu, C. (2019). Inflammation-related biomarkers in major psychiatric disorders: a cross-disorder assessment of reproducibility and specificity in 43 meta-analyses. Transl. Psychiatry 9:233. doi: 10.1038/s41398-019-0570-y
Yuki, K., Fujiogi, M., and Koutsogiannaki, S. (2020). COVID-19 pathophysiology: a review. Clin. Immunol. 215:108427. doi: 10.1016/j.clim.2020.108427
Keywords: coronavirus disease 2019, neuropsychiatric disease, cognition, depression, mental health
Citation: Kumar S, Veldhuis A and Malhotra T (2021) Neuropsychiatric and Cognitive Sequelae of COVID-19. Front. Psychol. 12:577529. doi: 10.3389/fpsyg.2021.577529
Edited by:
Gian Mauro Manzoni, University of eCampus, ItalyReviewed by:
Gregory Zecca, Independent researcher, Geneva, SwitzerlandJing Yuan, Children’s Hospital of Capital Institute of Pediatrics, China
Copyright © 2021 Kumar, Veldhuis and Malhotra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sanjay Kumar, skumar@brookes.ac.uk